Why You Treat the Symptom Instead of the Cause on NCLEX Questions
A patient is short of breath.
You reach for oxygen.
And you get the question wrong.
Why It Feels Right
In clinical practice, addressing the presenting symptom is often correct — and always compassionate. Patient is in pain: manage the pain. Patient is hypoxic: apply oxygen. Patient is anxious: reassure them.
This is responsive, attentive care. It's what you were trained to do.
Why It Fails on NGN
NGN doesn't reward treating the presentation. It rewards identifying what's driving it.
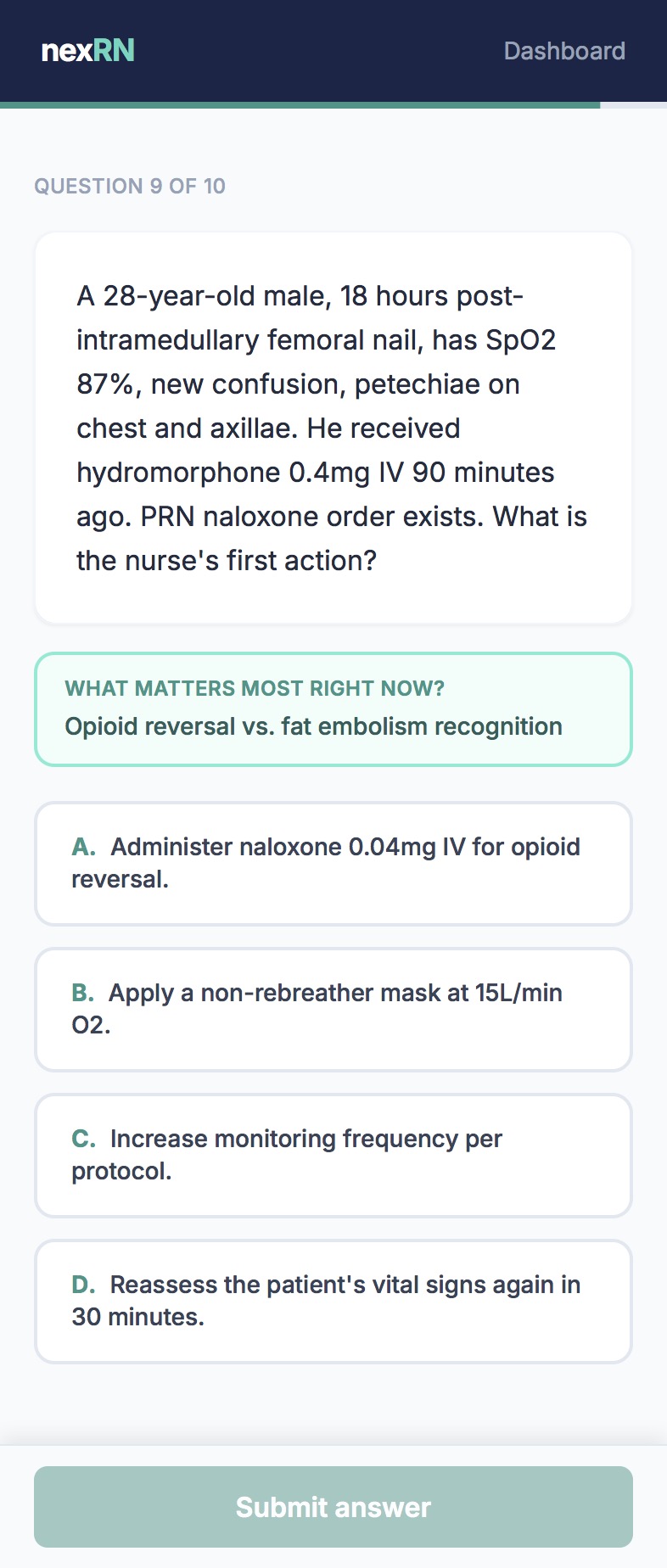
A patient who is short of breath could be experiencing heart failure, pulmonary embolism, pneumonia, anxiety, or anemia. Each requires a different priority action.
Treating the SpO2 without identifying the cause means you're managing a number, not a patient.
This is why students who know exactly what to do for each condition still prioritize incorrectly — they're reacting to the visible finding instead of asking what's causing it.
This is one of the most common patterns we see across thousands of sessions.
Pattern Identity
If you've been choosing answers that address the obvious finding — and getting them wrong — this is probably your pattern. The instinct to respond to what you can see is deeply trained. Most students don't realize they're doing it until they see it named.
What It Looks Like in Practice
The first student treats a number. The second student identifies a pattern.
Why More Questions Don't Fix It
You can do 500 respiratory questions and still default to treating the symptom — because those questions teach you what hypoxia means, not how to look past it.
Training the decision to search for the cause requires a different kind of practice.
nexRN trains the clinical judgment the NCLEX actually tests — 10 questions per session, every day.
Try a free session at nexrn.ai