Why You Prioritize the Wrong Patient on NCLEX
Four patients. One looks sick. One is quietly deteriorating.
You pick the obvious one.
You get it wrong.
Why It Feels Right
Abnormal vital signs were taught as action signals. High fever: investigate and treat. Tachycardia: monitor closely. The patient with the most obvious abnormality gets the first response.
That's attentive nursing. It's how you were trained to triage.
Why It Fails on NGN
NGN doesn't test current acuity. It tests deterioration trajectory.
The question isn't: who is sickest right now? It's: who is most likely to be in a crisis in the next 30 minutes if I don't intervene?
A patient with a stable fever at 39.2°C who has been febrile since admission is being managed. A post-chemo patient who is suddenly quiet and not complaining may be unable to communicate that they're crashing.
The silence is the sign. Students reading current status miss it entirely.
This is one of the most common patterns we see across thousands of sessions.
Pattern Identity
If you've been going to the most obviously abnormal patient — and losing prioritization questions — you're reading the snapshot instead of the trend. This is one of the most common patterns in students preparing for NGN.
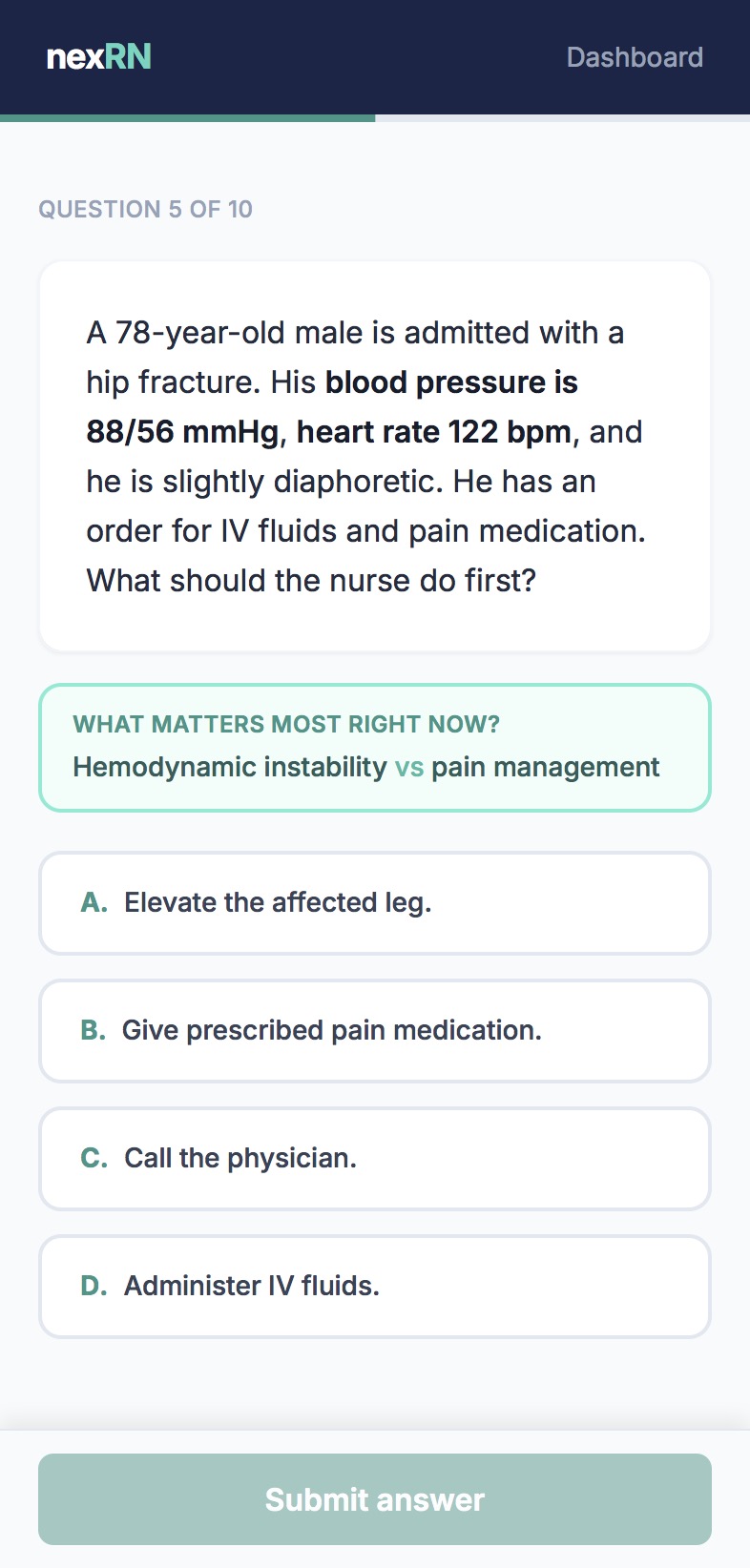
What It Looks Like in Practice
The first student responds to the obvious sign. The second student reads the clinical story.
Why More Questions Don't Fix It
Prioritization is one of the most-practiced — and most-missed — question types. Because practice questions reinforce recognition of abnormal values, not trajectory analysis. Volume doesn't fix a pattern that the practice system keeps reinforcing.
nexRN trains the clinical judgment the NCLEX actually tests — 10 questions per session, every day.
Try a free session at nexrn.ai